Given the increasing stress levels among medical students due to the impact of COVID-19, it is crucial to effectively reduce their stress levels for their future development. To better understand medical students’ stress coping, this study investigated how their emotional intelligence is related to stress coping and whether this relationship is moderated by gender differences.
A cross-sectional study was conducted. A random sample of 744 medical students from Hebei Province, China, was investigated via an emotional intelligence scale and stress coping questionnaire from March–May 2023. The response rate was 93%. SPSS and Mplus statistical software were used for the data analysis.
The current study revealed that gender is a significant moderator of the relationship between medical students’ emotional intelligence and stress coping. These findings may help medical colleges focus on gender differences when improving medical students’ ability to cope with stress.
College students are faced with many internal and external stresses that mainly come from academic, personal, and interpersonal relationships. Since COVID-19, the stress level of college students has increased [1]. This is especially true for medical students, who are more likely to encounter COVID-19-infected individuals [2]. Stress is regarded as a life crisis that affects the development of college students at all stages. High stress levels among medical students may lead to psychological problems such as depression, anxiety, and irritability [3, 4], which can cause serious harm to their physical and mental health [5]. Furthermore, it will have a certain degree of influence on the career planning of medical students [6]. Therefore, effectively reducing the stress level of medical students is highly important for their future development.
As a special group, medical students are also facing the pressure of changing from being college students to being qualified medical workers [7]. Thus, medical students face more pressure than students from other majors [8]. Stress coping involves the different ways people deal with stress. Many medical students try to eliminate or reduce the impact of stressors by using effective or ineffective styles to cope with stress [9]. As an intermediary mechanism of stress and health, stress coping has important protective effects on individuals’ physical and mental health. As a new force in the field of health care, medical students’ effective stress coping and maintenance of mental health have a crucial impact on their social development.
Previous research on stress often coincides with research on emotion, which is experienced both physically and mentally [10]. Emotional intelligence is the ability to recognize one’s own and others’ emotions, to motivate one’s own emotions, and to manage one’s emotions in interpersonal relationships [11]. Emotional intelligence greatly affects individuals’ behavior and performance [12]. It helps students select the most appropriate stress coping style [13]. In previous studies, emotional intelligence was shown to buffer stress through active coping [14, 15]. In other words, emotional intelligence minimizes the negative effects of stress and improves coping [16].
Gender has been shown to be an important factor that influences stress coping. Researchers have found that females tend to use behavioral coping more actively than males do [17, 18]. However, some scholars believe that, based on the socialization hypothesis, females are more likely to use avoidant coping, while males are more likely to adopt active coping [19, 20]. There is no consistent conclusion on the impact of gender on stress coping. These inconsistent findings highlight the need to consider gender differences when examining medical students’ stress coping.
Similarly, the study of emotional intelligence also emphasizes gender differences [21]. On the one hand, there are significant differences in the level of emotional intelligence between males and females [22]. On the other hand, gender has an important influence on the role of emotional intelligence [23]. Gender differences exist in both emotional intelligence and stress coping. However, to date, little research has been conducted on the potential role of gender as a moderator in the relationship between emotional intelligence and stress coping. As a moderator, the relationship between emotional intelligence and stress coping can still exist in the Chinese context, even in the absence of gender [15, 24]. Therefore, whether there is a gender difference in the impact of emotional intelligence on stress coping among Chinese medical students is worth further exploration.
Therefore, this study explored the gender differences in stress coping in the field of health care and further explored the role of medical students’ gender as a moderator of emotional intelligence dimensions on stress coping. Thus, the influence mechanism of emotional intelligence on the stress coping of medical college students is clearer. At the same time, we expand the research on the influence of gender differences on stress coping.
Individuals try to alleviate stress by reducing stressors, regulating negative emotions, and re-establishing their inner balance; in other words, they engage in coping [25]. The most commonly used definition of stress coping by Lazarus and Folkman is “constantly changing cognitive and behavioral efforts to manage specific external or internal demands that are far beyond the existing resources of the person” [26].
Researchers have typically divided coping into two styles: problem-focused coping and emotion-focused coping [27, 28]. However, some researchers have divided coping from the perspective of behavior into two categories: active and avoidant coping [17, 29]. Active coping involves considering ways to overcome stress and make plans for subsequent efforts, seeking social support and taking advantage of the situation by learning lessons from it [30]. Avoidant coping includes withdrawal and avoidance [31, 32]. This division is more concise and easier to understand and analyze. Therefore, to better guide practice, we chose this division.
Many scholars have proposed that emotional intelligence and stress coping are inseparable [15, 33]. An increasing number of articles have established a relationship between emotional intelligence and stress coping among students [16, 34]. These studies seemingly indicate that students with greater emotional intelligence display better stress coping.
In this research, we used Lazarus and Folkman’s definition of stress coping to explore the relationship between emotional intelligence and stress coping among medical students of different genders.
Emotional intelligence is related to an individual’s ability to deal with stress [24]. Emotional intelligence is the ability of individuals to recognize, evaluate, manage and control their own or others’ emotions [35]. The Wong and Law Emotional Intelligence Scale (WLEIS) is one of the most widely used measures of trait emotional intelligence. According to this measure, emotional intelligence includes an individual's specific ability in four aspects: (1) self-emotional appraisal, (2) others’ emotional appraisal, (3) use of emotion, and (4) regulation of emotion. Specifically, self-emotional appraisal relates to the individual’s ability to understand their deep emotions and be able to express these emotions naturally; regulation of emotion is the ability of people to regulate their emotions, which will enable a more rapid recovery from psychological distress; use of emotion is the ability of individuals to make use of their emotions by directing them toward constructive activities and personal performance; and others’ emotional appraisal is the ability to perceive and understand the emotions of those people [36].
With regard to stress coping, Moradi confirmed that people’s level of emotional intelligence helps in predicting useful stress coping [37]. Similar results were found in subsequent studies. Goleman argued that emotional intelligence includes traits such as motivation, optimism, adaptability, and warmth [38]. This adaptive capacity, also known as resilience, enables people to recover from stressful situations in the face of adversity [39]. High emotional intelligence is related to good adaptability [40]. In other words, students with high emotional intelligence have greater adaptability when facing stress. Due to their future occupation, medical students face more stress, so adaptability is necessary for them. Students with greater adaptability show a greater tendency to adopt active coping when faced with pressure and mental health problems [41].
In a study of college students’ stress coping, Fteiha reported a positive correlation between emotional intelligence and active coping [33]. Similarly, Por reported that individuals with higher emotional intelligence scores engaged in more active coping [42]. Based on the above discussion, the first hypothesis for this study is as follows:
H1: Emotional intelligence has a positive impact on the active coping of medical students.
Emotional intelligence is the ability to address one’s emotions, and an individual with high emotional intelligence is generally optimistic [43]. Optimistic students can see the positive side of the undesirable status quo and adopt active coping [44] instead of avoidant coping to escape stress.
According to a study of first-year law students, those with greater positive affect were less likely to adopt avoidant coping [45]. Similarly, many studies have shown that individuals with low emotional intelligence use more avoidant coping [24, 46]. Based on the above discussion, the second hypothesis of this study is as follows:
H2: Emotional intelligence has a negative impact on the avoidant coping of medical students.
Gender is recognized as an important predictor of differences in stress coping. The majority of prior studies found different results. Women believe that they do not have sufficient resources to cope with stress and tend to adopt an active coping style by seeking support from others [47]. Carver reported that women coped with stress positively by seeking social support, while men coped negatively by using distracting means such as alcohol and drugs [48]. Similarly, a recent study of law enforcement officers revealed that female officers were significantly more likely to use active coping, including emotional and social support, than male officers were [49].
However, the results remain somewhat mixed. Due to gender stereotypes, males are often associated with reason, while females are associated with emotion. According to Howerton, females are more likely to adopt avoidance-centered avoidant coping [50]. Another study revealed that females engage in more avoidant coping and that males engage in more rational active coping [51]. However, recent research has suggested that there are no statistically significant differences in the methods of coping with psychological stress based on gender [24].
Gender differences in stress coping can be explained by variations in the types of situations that female and male students typically encounter. Being female may be socially associated with exposure to a specific set of gender-related stressors, such as discrimination, battering, rape, and sexual harassment [52]. This may mean that different types of stress coping are needed.
Mixed results for the impact of gender on stress coping were found in the previous literature. However, the majority of related research suggests that gender differences have an impact on stress coping. Hence, we clarify the impact of gender differences on the stress coping of medical students. We propose the third hypothesis of the study:
H3: Gender moderates the emotional intelligence and stress coping of medical students.
Above literature reviews indicated that stress coping can be affected by gender and emotional intelligence. This research aimed to compare the associations between emotional intelligence dimensions and stress coping among medical students of different genders.
The study was mainly built on a quantitative design and survey research. This research adopted cluster random sampling. Hebei Province, a major province for the enrollment of medical students, was selected as the sampling area. Then, three medical colleges (enrollment number > 1200) were randomly selected from Hebei, as the medical colleges specialize in training medical students.
During the period of March–May 2023, we conducted a survey on the senior students of the two schools with the largest number of students in the three medical colleges, basic medical school and nursing school. The third author distributed the survey questionnaires to 800 Chinese medical students. Written informed consent was obtained from the participants after the researchers explained the purpose, risks, and benefits of the study, as suggested in prior research. Participation was voluntary, and no personally identifiable information was collected. In addition, at the beginning of the questionnaire, there was a cover letter containing information concerning purpose, anonymity, and confidentiality. The letter also included instructions and fill-in methods for those medical student participants.
The distribution of the questionnaires was completed in the classroom. The survey instrument included demographic conditions, the emotional intelligence scale and the stress coping scale and was distributed to each student by the researchers with the assistance of teachers. The questionnaires took approximately 20 min to complete. A questionnaire recovery box was set up in the college, and the participants completed the questionnaire and put into the box by themselves. After 56 invalid questionnaires were excluded, 744 valid questionnaires were finally collected, yielding an effective response rate of 93%.
All the measures were prepared in Chinese. The emotional intelligence scale was initially developed by Law K [53], and we used a Chinese version of the scale. To avoid distortion in the translation, the scale was independently translated back to English by two professionals and compared with the original English version. The scale has good reliability and validity in the Chinese context [54, 55].
Emotional intelligence. Students’ emotional intelligence was measured using the questionnaire adapted from Law K, which consisted of four dimensions: self-emotion appraisal, other-emotion appraisal, use of emotion and regulation of emotion [53]. The survey included 16 items rated on a five-point scale (from 1 ‘strongly agree’ to 5 ‘strongly disagree’). High scores indicate good emotional intelligence, and low scores indicate poor emotional intelligence. Sample items included “I truly understand what I feel”, “I always know my friends’ emotions from their behavior”, and “I always tell myself I am a competent person”. The internal reliability of this questionnaire was sufficiently high (α = 0. 859).
Stress coping. Students’ stress coping ability was measured using the Chinese version of the questionnaire adapted from Frydenberg, which consisted of two dimensions: active coping and avoidant coping [56]. The survey included 13 items rated on a four-point scale (from 1 ‘do not use’ to 4 ‘often use’). Sample items were “I do not take the problem too seriously” and “I try to forget the whole thing”. The internal reliability of this questionnaire was sufficiently high (α = 0. 893). The Cronbach’s α for active coping and avoidant coping was 0. 871 and 0. 889, respectively.
Control variables. The moderator of gender was measured as 0 = female and 1 = male. The other demographic variables included only child (1 = yes; 2 = no), major (1 = nursing major; 2 = anesthesiology major, 3 = medical imaging major, 4 = medical laboratory science major), origin (1 = countryside; 2 = town; 3 = city), and class leader (1 = yes; 2 = no). Previous studies have shown that demographic variables, such as origin and being an only child, are likely to influence emotional intelligence and stress coping [57, 58]; therefore, these variables were included as control variables.
In this study, the measurement scales were presented to the participants in the following order: demographic variables such as student gender, the emotional intelligence scale, and the stress coping scale.
The SPSS 26 statistical software package was first used for data analysis. The demographic characteristics of the sample are described as the mean (M), standard deviation (SD), number (n), and percentage (%), as appropriate. Group differences in stress coping ability were tested by t tests or one-way ANOVA. We then presented the means, standard deviations, and correlation values among the study variables. Because gender is a binary variable (female or male), we used group comparisons. We asked participants to self-identify their genders. After controlling for other demographic variables, Mplus 7.4 was used to compare the relationship between emotional intelligence and stress coping among students of different genders.
First, this study is the first to compare the connection between emotional intelligence and stress coping among medical students of different genders. This finding confirms that different emotional intelligence dimensions influence how medical students cope with stress. These comparisons indicate that medical students’ stress coping is complex and influenced by many individual factors. This study therefore contributes to the literature on medical students’ psychological health.
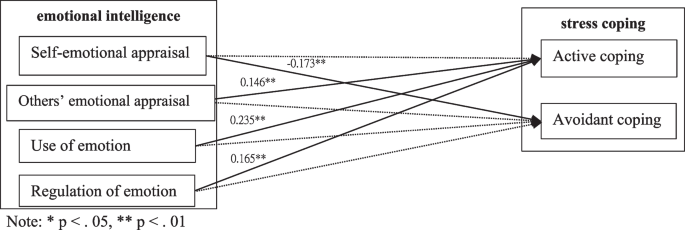
Second, the outcome of the current study confirms that self-emotional appraisal significantly negatively predicts both female and male medical students’ avoidant coping. Medical students with high self-emotional appraisal ability are more aware of changes in their emotional patterns, and they are also more likely to make plans and engage in active coping [59]. In other words, they will reduce the use of alcohol and other avoidant coping to vent their emotions. However, this finding is contrary to that presented by Jung and Yoon [34].
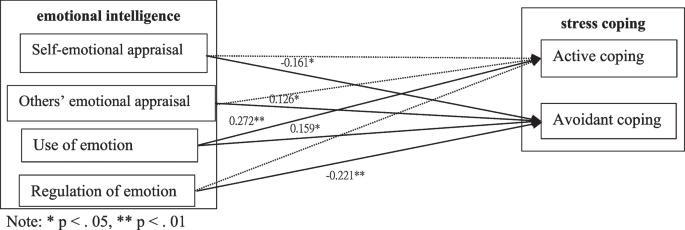
Additionally, the use of emotion was found to have the greatest impact on both female and male medical students’ active coping and to have positive and significant effects on male students’ avoidant coping. Students with high scores for the use of emotions will use emotions to relieve stress. There is robust evidence that positive emotions cooccur with negative emotions during intensely stressful situations [60]. Therefore, students can make full use of positive emotions and adopt positive coping styles. It is also possible to avoid coping due to the guidance of negative emotions. Compared with females, male medical students are less able to identify their negative emotions [61], resulting in their inability to use negative emotions correctly. Thus, male medical students are more likely to avoid coping under the guidance of negative emotions.
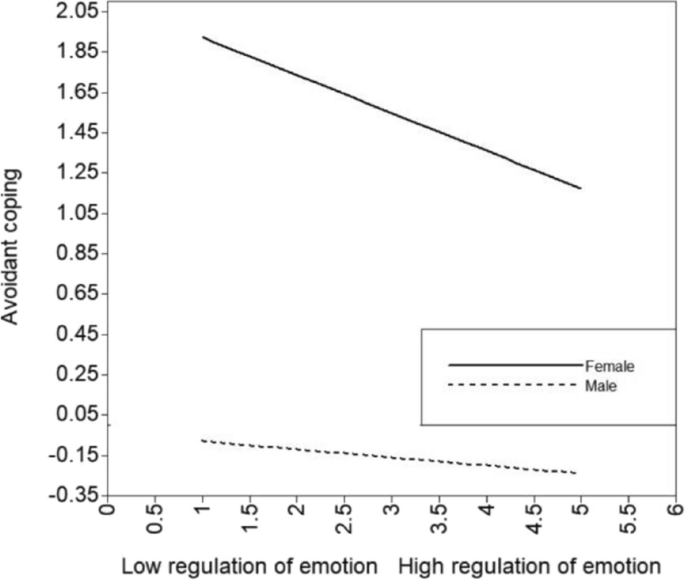
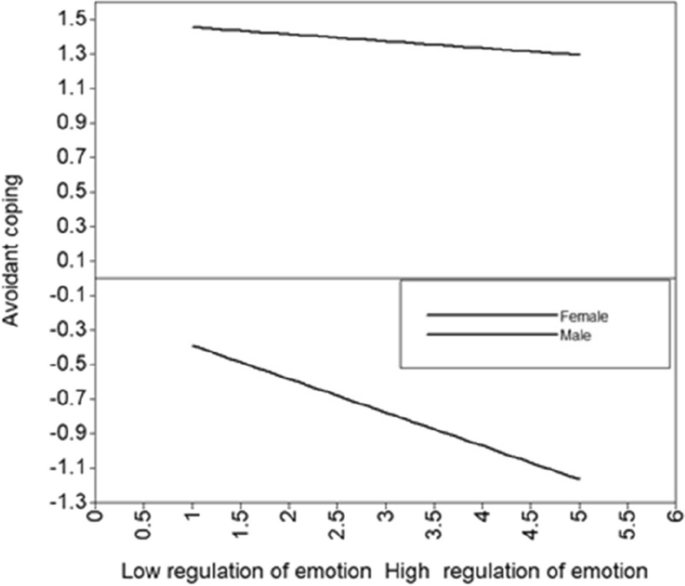
Additionally, the regulation of emotion significantly positively predicts female medical students’ active coping but significantly negatively predicts male medical students’ avoidant coping. Regulation of emotion is the ability of people to regulate their emotions. In other words, medical students with high regulation of emotion ability have greater adaptability [10]. They are more likely to face stress when they have a positive and optimistic attitude. Thus, the ability to regulate emotion helps female students cope more actively and helps male students cope less effectively. This conclusion is consistent with the literature, which indicates that an increase in the regulation of emotion increases the use of active coping [15, 24, 34]. However, in contrast to Eschenbeck’s results, no gender differences occurred for stress coping related to emotion regulation [62].
Fourth, others’ emotional appraisal significantly positively predicts female medical students’ active coping. Females pay more attention to participating in social activities [63], and females are more likely to seek social support to reduce stress [64]. Thus, students with greater emotional appraisal can better ‘read’ the environment and others’ emotions and respond accordingly to obtain more social support when faced with stress. Videlicet, they will cope more actively. This finding is consistent with previous research findings showing that females cope more actively to relieve stress [49, 65].
However, for male medical students, others’ emotional appraisal has statistically positive and significant effects on avoidant coping. Male students who score higher in others’ emotional appraisal are more sensitive to others’ emotions, which leads them to bear more pressure [66]. Males are more independent and rarely seek help in the face of pressure [67]. This leads them to engage in more avoidance coping.
Finally, when comparing the influence of the emotional intelligence dimensions of students of different genders on their stress coping, our research indicates that female medical students’ others’ emotional appraisal has a much greater effect on active coping. This may be because under the influence of traditional Chinese culture, the expectations of males and females are different, males are more independent and more responsible, and females are more sensitive and more careful [68]. Thus, compared with male medical students, female medical students are more sensitive and concerned about the emotions of others. In other words, female medical students are more careful than male medical students in interpersonal relationships. This makes female medical students’ friendships more active, intimate, and emotionally supportive [69]. Thus, high others’ emotional appraisal helps female medical students maintain a better interpersonal circle and obtain more social support. When female medical students face stress, they are more likely than male medical students to use help-seeking behaviors to actively cope [39].
Furthermore, male medical students’ regulation of emotion had a stronger effect on the reduction of avoidant coping. This may be because tobacco use and alcohol consumption are greater in males than in females in China [70]. In other words, when facing stress, males are prone to think of using avoidant coping, such as smoking and drinking, to relieve stress, while females usually do not. Therefore, because females use less avoidant coping, better regulation of emotion has less of an effect on avoidant coping. In contrast, for male medical students, the ability to regulate emotion helps them to better restrain negative feelings and, in its place, promote positive feelings such as confidence, empathy and friendliness [71]. This helps male medical students face stress with optimism, so they will take the initiative to find a solution and take less avoidant coping.
In general, although female medical students suffer more stressors and are more likely to be affected by stressors [72], we have found that emotional intelligence can better help female medical students relieve stress than can male medical students.
This research contributes to the empirical investigation of stress coping in several ways. First, we confirmed the moderating effect of gender. Previous studies have reached different conclusions about gender differences in stress coping [18, 20]. Moreover, few studies have focused on gender differences in stress coping in the Chinese context. In China, medical students are under great pressure. We examined gender differences in stress coping and identified inconsistencies in previous studies. This study fills the gap in the literature on gender differences in the stress coping of medical students in the Chinese context and helps Chinese medical students better relieve stress.
Second, previous studies have shown that there are gender differences in emotional intelligence and stress coping. However, few studies have tested gender differences in the effect of emotional intelligence on stress coping, which represents a serious gap in the literature. Thus, we have comprehensively promoted the research progress on gender differences in these two fields rather than studying gender differences in emotional intelligence or stress coping in isolation. This can better guide medical students to relieve stress.
Furthermore, in previous research, stress coping strategies have been divided into two categories: problem-focused coping and emotion-focused coping. We divided stress coping behavior into two categories: active coping and avoidant coping. This division is more concise and easier to understand and analyze, so our results can better guide practice.
The results of this study have many important implications for college education, particularly for medical majors. First, the results of this paper shed light on the complex ways in which emotional intelligence is relevant to Chinese medical students’ active stress coping. Colleges should offer mental health courses so that medical students can maintain a positive and optimistic attitude and can adopt more effective active coping in the face of pressure.
Second, given the larger proportion of female medical students, the results showing that gender differences moderate the effect of emotional intelligence on stress coping could provide an effective solution for college students. Colleges can increase medical students’ emotional intelligence skills through courses and practice, particularly for female students. This can improve students’ emotional intelligence and help them actively cope with stress to relieve their stress and anxiety. A healthy psychological state has a crucial impact on future doctors and nurses.
Finally, according to Damla, seeking social support is the most common stress coping style among doctors and nurses [73]. Social support is provided by networks comprising family, relatives, and friends. Thus, colleges should encourage students to socialize and make friends. At the same time, colleges should regularly communicate with parents to provide necessary support for students.
There are some limitations of this study that may affect the results. One potential limitation is that all variables were measured by self-reports, which may have led to response bias. To overcome this weakness, multiple indices (e.g., physiological and physiological indices) should be used to obtain more reliable information about the emotional intelligence levels of participants in the future.
Second, all the participants in the study were from 3 regions in Hebei Province and from 3 medical colleges. Medical colleges in other provinces were not investigated. The sample data we used may not be sufficiently comprehensive. Future research should attempt to select more colleges by expanding the geographical scope and especially focusing on colleges in first-tier cities to compare the effect of different levels of economic development on students’ emotional intelligence and stress coping. In addition, there are still some important sociocultural factors that we do not take into account. Thus, attention to other variables, such as Chinese culture, is also one of the future research directions.
Finally, we use a cross-sectional study, and only preliminary inferences are made on the relationships between variables. It is impossible to clarify the causal relationships between variables. Tracking research design or experimental research is still needed to further improve the paper.
The results show that the different dimensions of emotional intelligence have different effects on the active/avoidant coping of medical students of different genders. In addition, there are gender differences in the impact of others’ emotional appraisal on active coping and the impact of the regulation of emotion on avoidant coping. This study provides compelling evidence that focusing on gender is useful for improving medical students’ stress management skills. Therefore, different interventions for medical students of different genders are beneficial for increasing the impact of emotional intelligence on stress coping and can be used to help medical students relieve severe stress.
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
The authors thank all the participating medical teachers and students. We would like to express our gratitude to them for their assistance.